Ivor Cummins: Evaluating some European unconventional doubter/denier viewpoints
- Jeffrey Morris

- Sep 9, 2020
- 13 min read
Updated: Nov 30, 2020
This video by Ivor Cummins describes some of his unconventional viewpoints. He supports the position that mandatory lockdowns were not needed, and has a hypothesis that viral deaths are cyclic suggesting that countries that were hit hard by flu before 2020 did not have as many deaths from COVID-19 while those with low flu death rates in 2019 had higher COVID-19 deaths.
This was forwarded to my by a friend so I watched and gave my thoughts to him, and since I was so detailed thought I would turn it into a blog post since his ideas highlight several important points about our society and this pandemic, and the doubter/denier vs. worrier/alarmist ends of the continuum on COVID-19.
1. He highlights some real facts that for some reason don't seem to register with many individuals in our society or the media -- these are facts that people on the doubter/denier end of the spectrum focus on. Some of these are real facts, and need to be acknowledged and understood if we are to have full knowledge of what is going on in the pandemic and to construct the best mitigation and management strategies. Some of these facts are not acknowledged by many who tend towards the alarmist end of the continuum. Ignoring these facts feeds the denial/doubter perspective.
2. While acknowledging these facts and bringing some interesting ideas to the discussion, he seems to ignore other facts and data, effectively cherry picking information to support his thesis. I will point out some of these problems with his argument and what information he is not taking into account.
First, I will highlight his points that I agree with:
1. The media has misrepresented the strategy and outcomes in Sweden -- they never really were seeking herd immunity -- i.e. they did not try to speed viral spread through society to reach immunity. Rather, their strategy was to avoid government mandated lockdowns, instead focusing on providing guidance to the public about targeted mitigation strategies and trusting them to follow them, which they largely have, much better than the USA has since reopening after lockdowns. He rightly points out that Sweden's death rate is far lower than what was predicted, and lower or comparable to many other European nations including UK, Spain, and Belgium, or the USA. Here is the comparison that shows that even with their controversial strategy, they are in better shape than the USA.
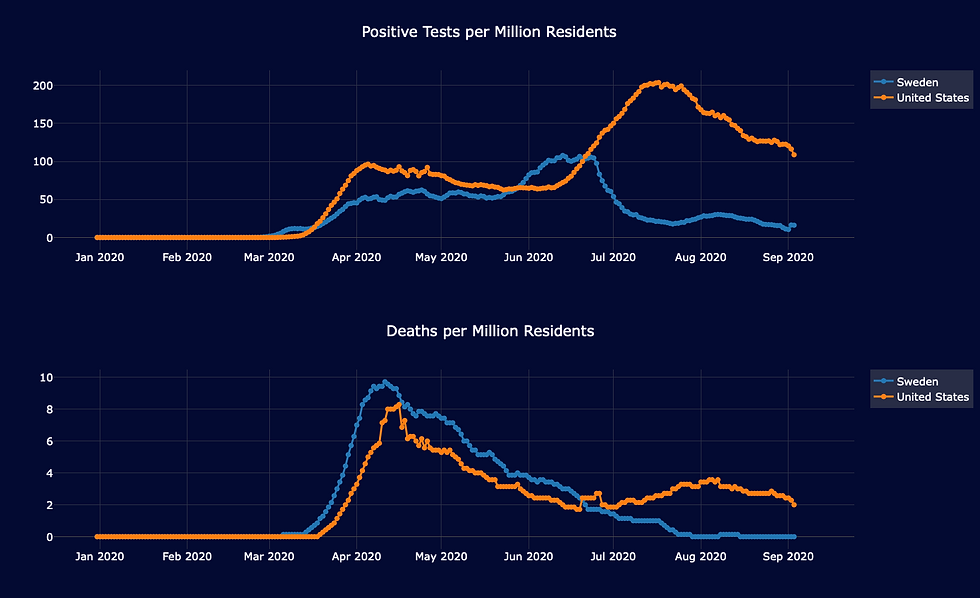
This is not to say I agree with their strategy -- I don't -- but it does bother me that they are such a media punching bag, and their approach and results are not accurately represented. I agree with this point that he makes.
2. People are obsessed with following numbers of cases and don't look enough at hospitalizations, deaths, and long term morbidity induced by the virus. When you look at those you get perspective on the virus, and can have a realistic sense of the risk of the virus to each infected person, which is important to have a complete picture of the effects of the virus.
3. It is important to consider the collateral damage caused by strict mitigation strategies, in terms of lives, public health, mental health, education, and the economy. These don't seem to be explicitly considered in people's discussions about strategies for viral control -- ideally policymakers would bring together multidisciplinary teams including infectious disease experts, but also other professionals including mental health professionals, educators, economists, and data scientists to try to pull together all of this information in a meaningful and explicit cost-benefit analysis.
4. I agree that there may be a subset of the population that have some T-cell memory from previous coronavirus infections from strains that are part of the common cold, and these may confer immunity or mild disease on these people. I am working on a blog post discussing key points from the literature about what we know and don't know about this phenomenon. It is largely ignored by many people in society, especially those leaning towards the alarmist side, and overemphasized, exaggerated and misrepresented by many leaning towards the doubter/denier side.
5. I agree there may be reasons why cases in the summer are more mild than the ones we will see in the fall and winter. There are many good reasons for that, the most convincing which involves lower viral loads -- high enough to lead to infection but not high enough to have as high a risk of severe infection as in the winter/spring time. The flip side of this is that all of the low death and hospitalization rates relative to April may increase greatly as the weather turns in the fall (which is another reason why I think getting viral levels under control right now is of paramount importance).
6. He mentions that places that had high death rates from COVID-19 strongly tended to have very low death rates for the 2019 flu season, suggesting this provided a population of vulnerable people. This is an interesting hypothesis, and he shows some plots -- would be better to see more rigorous study to be sure the effect is not cherry-picked from certain locations where it fits while ignoring other locations for which it does not.
In spite of my agreement with some of these points that I think are under appreciated by many and underreported in the media, I see a number of speculative arguments he makes without support, untested assumptions, and cherry picking science and representing himself like "he knows the real science" and studies he doesn't mention are somehow more flawed than the ones he chooses to focus on. I will give examples below. But first I will mention the key feature of his argument -- He ONLY looks at deaths, not cases, testing, hospitalizations, long term side effects from infection, with a few cherry picked exceptions to support specific points ...
I agree that deaths are ultimately most important from a human perspective, but they are not the only important thing, and they are the least reliable measure of epidemic viral spread. He does not mention potential long term complications for infected, which I will mention below could be a major issue and sufficient reason alone for caution. Deaths lag cases by a month or more, so during the early days of a surge we don't immediately see the deaths -- given the surges take a month or so until the cases are really high this means the correponding deaths will manifest maybe 2 months into the surge. This cuts into a lot of his argument that the European uptick in late summer will not produce a corresponding uptick in deaths like the Southern/Western USA summer surge did, instead speculating these cases do not indicate a true surge but rather speculating they are due to "false positive tests", "detecting nonactive virus", and "over-testing". Why is the surge happening now and not in June or July then? He never presents any plots overlaying testing to provide support for this -- in the Spanish pandemic, testing has steadily increased since May, yet cases stayed flat through August and then started a sharp uptick that is faster than the increase in testing. His argument here, that (a) the increase is artifact of testing and (b) it is not real because deaths haven't increased (much), is eerily similar to the specious argument made in Texas and Florida during their surges, where deaths predictably sharply increased after the usual delay. He never considers that the uptick in Spain and other European countries might not be a meaningless seasonal effect, but might be the beginning of a surge induced by people getting sick of staying at home and getting together indoor in crowds and starting a surge like happened in the summer in the southern USA -- that seems like Occam's razor (the most parsimonious explanation) to me. To understand this pandemic, it is necessary to look at all the data together -- including tests, cases, hospitalizations, severe disease rates, and deaths so an analysis based only on deaths misses insights into the dynamics of viral spread, which paint a lot more clear picture into what the pandemic is doing at a particular location.
Some of his speculative assumptions without support:
1. He blithely states that about 20% of populations were infected and then the death numbers came down predictably because 80% have T-cell immunity from "one of the many" other coronaviruses. First, only in the most highly surging places is it possible 20% were infected (Texas, Phoenix, Florida and NY in USA, Italy and Spain in Europe, e.g.). Second, assuming that all of those not infected in the first wave have "T cell immunity" is major speculation and implausible. For one thing, almost all these places locked down so many people were never exposed, especially vulnerable populations, and second, there is no evidence that 80% of the population has T-cell immunity. Third, the "many" coronaviruses he refers to are 3 that are part of the common cold, plus SARS/MERS that are rare in Europe or USA. Fourth, there are small studies that show evidence that 20-50% of the population have some T cell memory pre-SARS-CoV-2 and it is true that these may confer immune advantages to these individuals. Whether it confers actual immunity or just predisposes them to more mild disease is not clear, but there is no evidence this number is 80%.
2. He assumes the lockdowns, mask wearing, and physical distancing had no effect when he has little basis for doing so -- almost the entire world locked down for a time and after opening have had major physical distancing guidelines and most places have closed places with large indoor gatherings. He has no control group to which to compare in order to make this inference. From what we have learned in rigorous studies about how this virus spreads, it is clear that mitigation strategies like avoiding crowded indoor settings, physical distancing when indoors, and mask wearing make a clear difference in suppressing viral spread. Looking only at deaths before/after directives were made is not helpful in the least bit -- deaths depend on so many other factors and there is confounding of viral levels and time -- that make causal inference on these factors extremely difficult -- and his analysis did not even attempt to use the tools of causal inference in addressing this question, but cites a handful of selected studies and makes an argument about plots before/after directives were put into place.
3. He invents several concepts and terms without defining them or supporting them in scientific literature.
a. He says that the "virome does what it does", meaning that cases wax and wane with humidity, UV and seasonal immune cycles and ignores human intervention. What is virome and where is his support for this claim? There is a mountain of data showing viral spread is linked to societal behavior in terms of gathering indoors and physical distancing. This idea of the virus spreading based on season and not human behavior is antithetical to the principles of infectious disease.
3b. He says that by trying to limit the spread of the virus in the summer, we have interfered with the "ancestral/evolutionary safe summer spread immunity", of course without precisely defining or citing articles about this concept. He then claims that "there will NOT be a surge of deaths in the winter since any deaths will be what would have happened because of seasonal flu" and then out of the other side of his mouth claims "any extra deaths will be due to the summer mitigation strategies interfering with this natural evolutionary protection". Pretty slick, he can claim he was right whether there is a surge of deaths or not. This is perhaps the most transparently weak part of his argument.
4. He argues that "40 years of science" show masks don't work -- yet those were done for flu and other respiratory viruses that don't spread asymptomatically. It is clear from what we have learned that one of the key characteristics of SARS-CoV-2 is that it spreads predominantly from asymptomatic/presymptomatic infected which is what makes it so hard to get its spread under control. This is precisely why masks are recommended in this case but not for flu. There is ample evidence from designed mechanistic experiments that even cloth masks block a high % of the particles exhaled by infected individuals, and given most spread is from respiratory particles it stands to reason that this would slow (not completely prevent) spread. And there is epidemiological evidence to support it has an effect although as above difficult to show causally. Since masks are easy and harmless to wear, especially when indoors around other people, it is staggering to me why some people have such an aversion to them as a basic mitigation strategy.
5. Throughout he equates flu to SARS-CoV-2, and it is clear this is his ideological perspective that "this is no more than a flu that has been overhyped". This is fundamentally wrong, as there are numerous features of SARS-CoV-2 far more problematic than flu -- from its proclivity to super-spread and spread from asymptomatics to the broad immune system/inflammatory disregulation it can induce that leads to severe cases and deaths. These problems also lead to post-infection inflammatory syndomes ,in some children, and apparent serious lasting side effects from infection such as the documented myocarditis that has been found in a sizable % of recovered people, especially young people, and including many people with asymptotic and mild symptom disease. If the numbers from this and other similar studies are representative, and if this is long-lasting, this could be a life-changing and major life-shortening after effect of the infection and a game changer that justifies extreme caution. We need to learn more, but this is the problem -- he is presuming there are no such effects or problem when all he looks at is deaths, and this virus works in freaky ways like nothing I've ever seen, and until we can confirm there are not major long term repercussions like this it is prudent to restrict infectious spread as much as possible, which he would dismiss as unnecessary or even harmful.
6. He presumes that all the death curves can be explained by natural seasonal variation like flu. This is convenient since most early surges happened in north in late winter which fit the timing. But the southern/western USA surge doesn't fit that at all -- and he blithely reclassifies this as "Mexico-like" and lumps this pattern in with Mexico and South America like it is a normal pattern. Yet he never shows from previous years that flu has this pattern in the southern USA because .... it does not. The easier and empirically supported explanation is that the southern/western USA surge happened later because (1) the initial surge was focused in NYC and didn't hit the south right away and (2) the south quickly and rather recklessly reopened putting lots of people together in crowded indoor settings and without masks, because these regions reject mask wearing, during the hot summer when people are indoors in AC to avoid the heat. This is much better explanation than his "virome" or "flu seasonal pattern" hocus pocus, and far more empirically supported from the data.
7. He simultaneously argues that the death curves from this covid-19 surge, which has been met with near universal lockdowns followed by physical distancing and mask wearing upon opening, has been "not that bad" comparing it to a usual flu season while simultaneously arguing that "lockdowns, masks and physical distancing don't work" without having a valid control or counterfactual against which to compare it. Sweden does not provide a valid counterfactual since, while they did not lock down, they closed secondary schools and recommended major physical distancing practices and encouraged outdoor gatherings, where it is beautiful weather in the summer so conducive to being outdoors. Sweden practiced what he called "smart distancing", and which I call "targeted mitigation". The counterfactual necessary for his analysis would be a society plowing through life ignoring the pandemic, not having lockdowns or mask wearing or closing anything, but also with people not taking any individual precautions like staying at home more, gathering outside instead of inside, practicing better hand hygiene and physical distancing, which would be like a typical flu season. The best simile to that is NYC in April and we saw how bad that went. If some place did THAT and the deaths were like flu, I might buy it, but all over the world we took all of these precautions and still saw these numbers of deaths. I believe had this counterfactual been followed the deaths and severe cases would have FAR dwarfed any flu season. He never acknowledges this potential bias because he conveniently and with very little evidence dismisses that any of these measures suppressed spread, while ignoring the volumnous scientific literature and entire infectious disease community and what they have learned about infectious disease throughout history. By ignoring the potential that death rates would have been much much higher without mitigation strategies, he can spin the relatively low death rates as nothing more than a "typical flu season". If his presupposition that mitigatoin has NO effect on cases and deaths is not true, then his whole analysis that the deaths are nothing more than a typical flu season also go out the window with it. It is appropriate that he ends his video with a diagram of a train of dominos, since if you push one domino of his untested assumptions over much of his argument goes along with it.
In conclusion, I'd say that he has some good points that need to be heard, but he goes too far trying to squeeze the data and pandemic into his preconceived explanations, which he presents in a condescending "I know what real science is" way, and makes speculative unsupported points, ignores data and studies that don't suit him, and does not even attempt to link the other data types into his analysis which is convenient because it is easier to spin his narrative using just the death data.
It makes me sad, because some of his key points I believe are valid and NEED to be heard -- the media and others DO have a blind spot that tends to push them towards the alarmist side, discounting evidence that paints the virus as not so foreboding and also skewing discussion of points like low mortality rate for most groups of people, the potential of T-cell memory assisting immune response for many people, and and honest assessment of Swedish strategy of experience and its lessons. But by going too far into speculation and cherry picking to tell a clean, compelling narrative (which he does well), he lowers himself to be nothing more than a partisan feeding the denier/doubter side, likely to be dismissed by people leaning towards the alarmist side or people in the middle.
Conversely, I think the failure to acknowledge some of these points mentioned above, perhaps driven by fear of somehow providing justification for the doubter/denier perspective, backfires and contributes to out inability to come together as a society and agree on a set of common facts that could serve as the basis for a unified strategy.
This is a shame because what we need is people illuminating some of the points he has made in a balanced way while acknowledging (1) how fast this virus spreads (2) that it does nasty things beyond a common flu, and we don't fully know all it does, (3) that mitigation strategies do slow viral spread, and thus suggesting that we should take some steps to slow its spread, but finding a middle ground that provides the best viral suppression possible while also minimizing collateral damage to society. If he made that balanced argument I think he'd be more influential to the people who don't already agree with him before they see his video podcast.



A patio cover provides valuable protection against harmful ultraviolet rays from the sun. Prolonged exposure to UV radiation can cause skin damage and increase health risks. By creating shaded areas, patio covers offer a safer environment for https://griffindeck.com/services/custom-decks outdoor activities. Families can spend more time enjoying their patios while reducing direct sun exposure. This added protection contributes to greater comfort and peace of mind during outdoor relaxation and entertainment.
A Baby Adoption Program can positively impact society by providing children with stable family environments. Research consistently shows that Single Parent Adoption supportive homes contribute to healthy emotional, educational, and social development. Adoption helps reduce uncertainty in children’s lives and offers opportunities for growth. Families created through adoption enrich communities by demonstrating compassion, commitment, and resilience. These positive outcomes highlight the value of responsible and ethical adoption practices.
He pushes us to see beyond just case numbers to the happy filled glass of nuanced data, like collateral damage on mental health, which we often overlook when fixated on fear.
This was an interesting and thought-provoking analysis that presents different viewpoints in a structured and balanced way. I appreciate how the post encourages readers to consider multiple perspectives rather than accepting simplified conclusions. It’s the kind of discussion that benefits from careful reading and critical thinking. In a separate context, I’ve seen references to https://grandoaksorthodontics.com/, which also emphasizes precision and evidence-based approaches in its own field. I recently came across a similar discussion on a review blog, and it offered an interesting perspective as well.
The way you presented complex information so simply is remarkable. I admire your ability to convey such detailed information in an accessible way. TADC Dating Sim